HOME
GLAUCOMA
What Is Glaucoma
GLAUCOMA RESEARCH AND CLINICAL STUDIES
Glaucoma Patient Stories
10 Things You Must Know Before Choosing Your Glaucoma Surgeon [Slideshare]
All Glaucoma Articles
TREATMENTS
Minimally Invasive Glaucoma Surgeries (MIGS)
Trabeculotomy
MIGS
Ab-Interno Canaloplasty
MicroPulse® P3 Cyclophotocoagulation
Endocyclophotocoagulation
Subconjunctival Implants
Suprachroidal Implants
Trabecular Bypass Implants
Trabectome
Non-invasive Glaucoma Surgeries
Laser Cyclophotocoagulation
Introduction To Laser Trabeculoplasty
Laser Trabeculoplasty – Additional Resource
Ultrasound Treatments for Glaucoma
Lower Risks Incisional Glaucoma Surgeries
Ab-Externo Canaloplasty
Penetrating Incisional Glaucoma Surgeries
Glaucoma Drainage Devices
Trabeculectomy
GLAUCOMA MEDICATIONS
How To Place Eye Drops In Your Eyes
Devices Created To Help You Get Eyedrops In Your Eyes
GLAUCOMA ALTERNATIVE TREATMENTS
Holistic Approach To Glaucoma
Glaucoma Supplements and Eye Surgery
Glaucoma Supplement Therapy Guidelines
IN THE PIPELINE
CANALOPLASTY
Canaloplasty Approaches
Ab-Externo Canaloplasty
Ab-Interno Canaloplasty
ReSGu Canaloplasty
Canaloplasty FAQs
Canaloplasty FAQ [Blog]
Canaloplasty FAQ [Videos]
Canaloplasty FAQ [Slideshare]
Canaloplasty Patient Stories
Canaloplasty In The News
Canaloplasty Surgery Videos
ARCHIVES
ABOUT
Contact Us
Map
Dr. Richardson’s Website
HIPAA Privacy Guidelines
Select Page
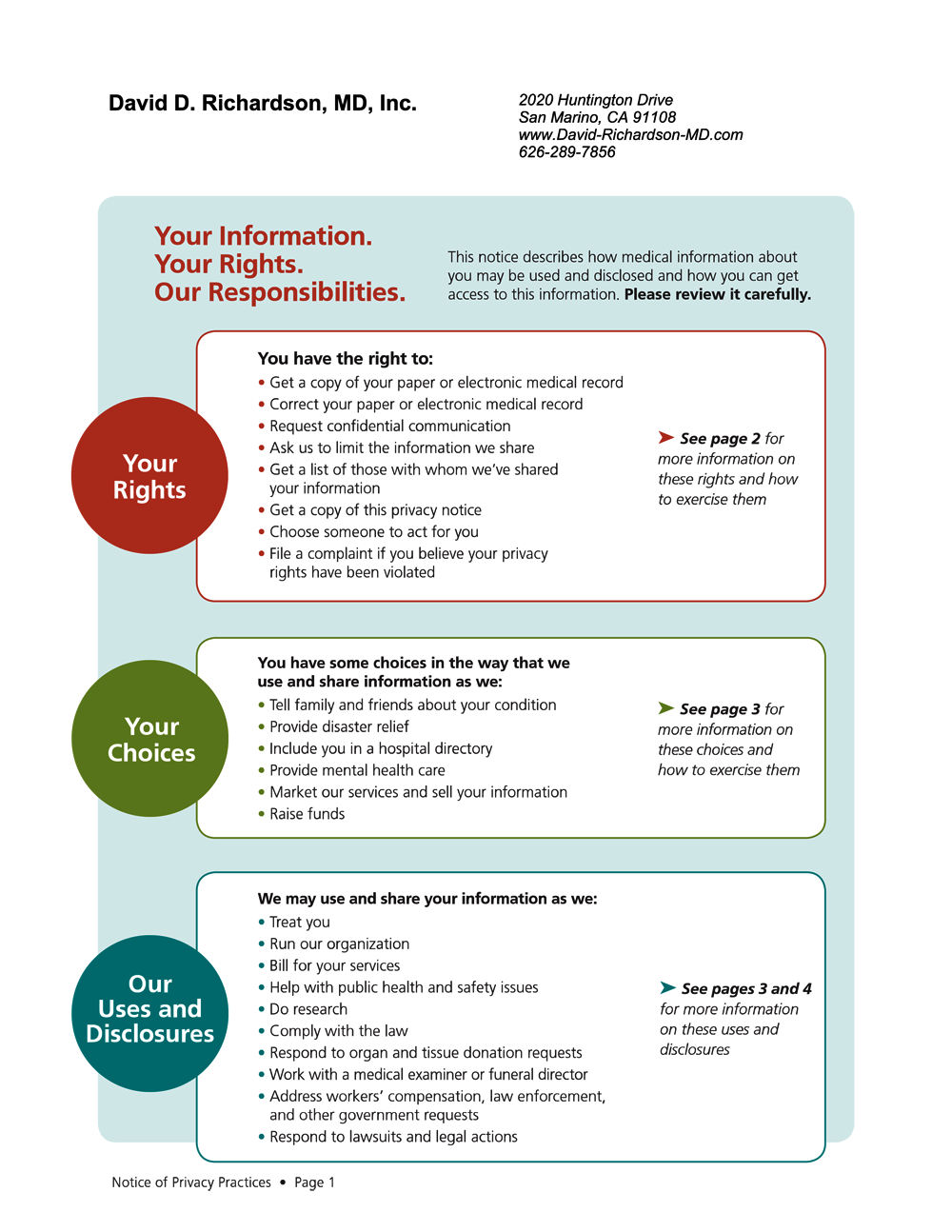
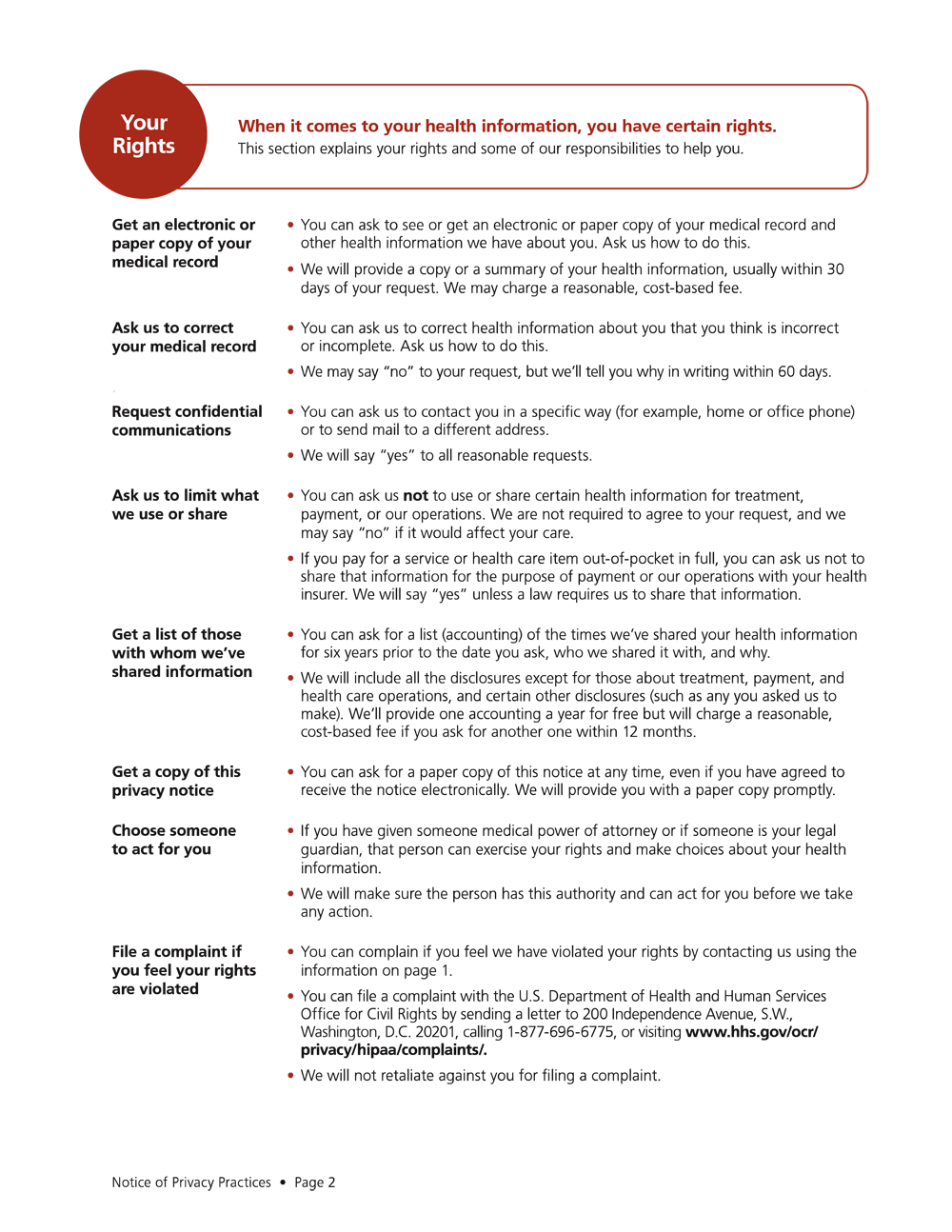
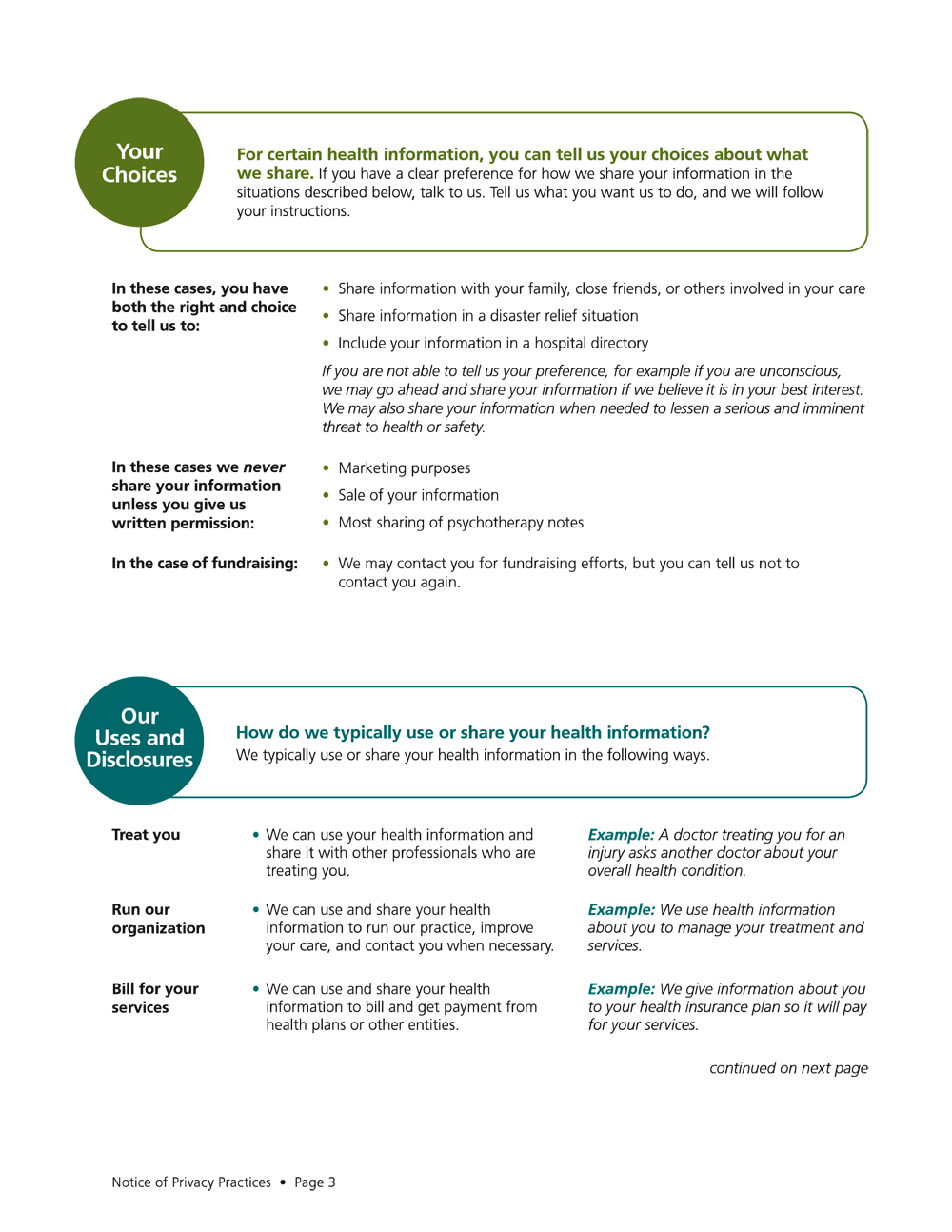
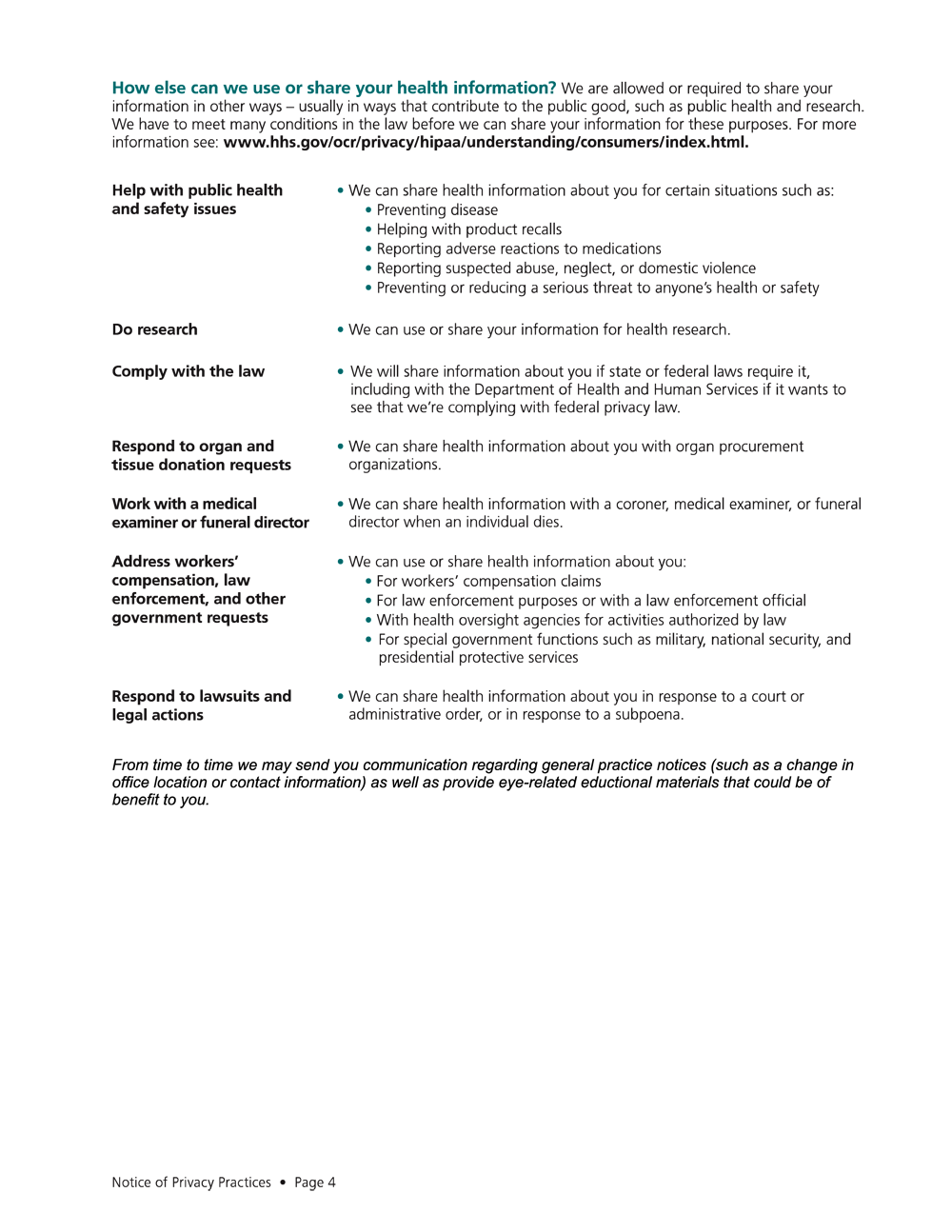
HIPAA Privacy Guidelines
Download HIPAA Privacy Guidelines (PDF Copy)
Pin It on Pinterest
Share This Page
Share information about glaucoma with your friends and family!
Facebook
Twitter
Pinterest
LinkedIn
Gmail